
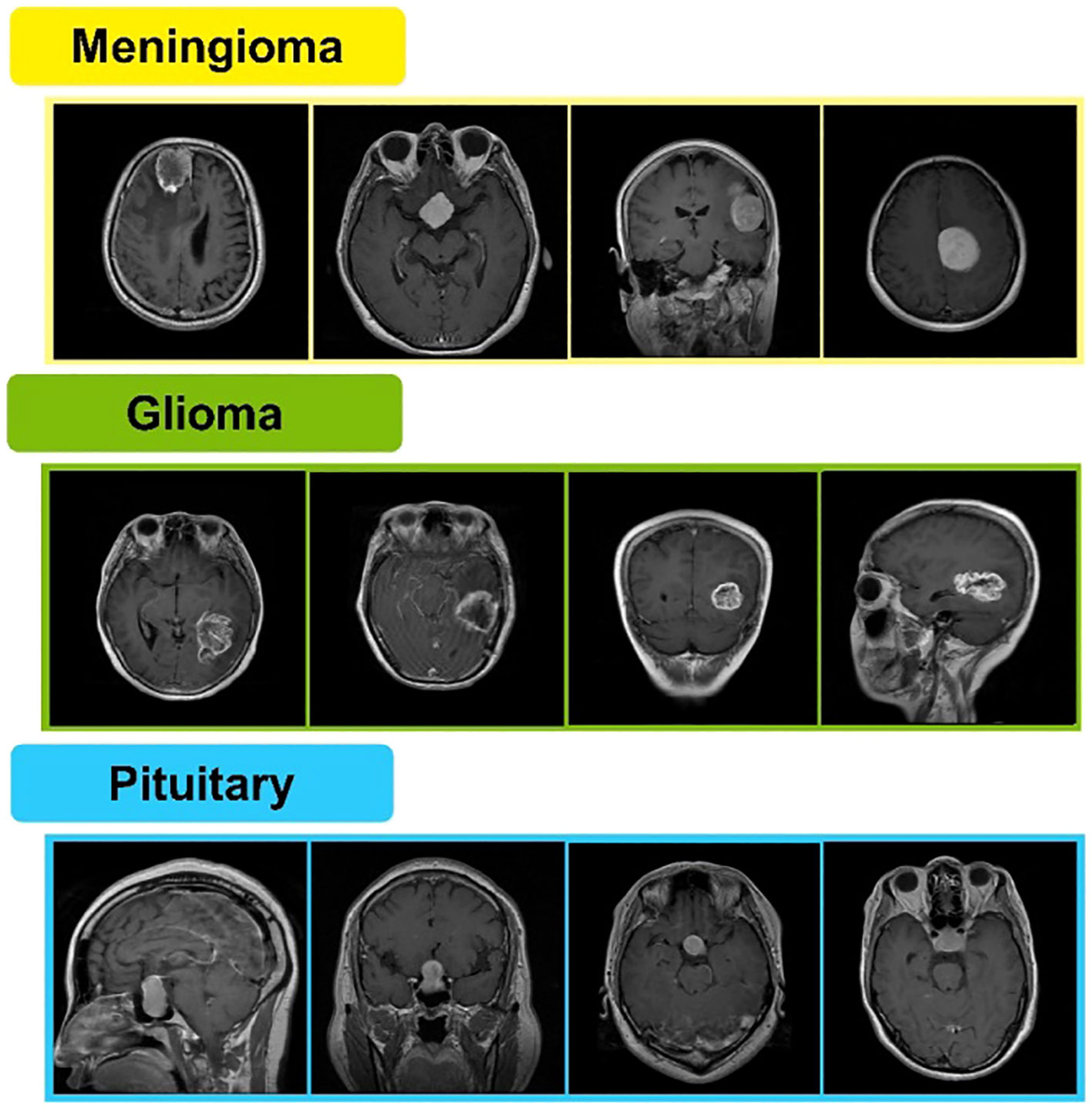
In the high-stakes field of diagnostic AI, headlines touting near-perfect accuracy are becoming routine. The latest paper, posted to the bioRxiv preprint server on May 28, 2026, makes just such a claim: a novel hybrid ai in medical detection method achieved an impressive 97.8% accuracy in classifying brain tumors on MRI scans. This model, which combines a Deep Convolutional Neural Network (DCNN) with a Whale Optimization Algorithm (WOA), has created a stir.
Table of Contents
But, as investigative analysts, we must ask the essential questions. Does this represent a verifiable breakthrough poised for clinical adoption, or is it another case of a lab-only success story? This report digs behind the numbers to separate the promising science from the premature hype surrounding the latest the technology developments.
The Current Landscape of AI in Oncology
To understand the significance of any single study, it’s essential to map the broader industry. The field of AI-driven medical imaging is not new; it’s a highly competitive space dominated by tech giants and specialized academic centers. Companies like NVIDIA have invested heavily in platforms like MONAI (Medical Open Network for AI), an open-source framework built on PyTorch to standardize and accelerate AI development for healthcare. This initiative involves a global consortium of institutions, including King’s College London and Stanford University, aiming to create reproducible, high-quality tools for clinical AI.
Read also: Humanoid robot: A Critical Analysis of the Mass Production Hype
The real moat in this sector is not merely a clever algorithm. It is fundamentally about two things: massive, high-quality datasets and the immense computational power to process them. It is well understood that an AI model is only as good as the data it’s trained on. A model trained exclusively on scans from one type of machine or a single patient population may fail spectacularly when deployed in a different hospital. This data-dependency is the central challenge for any new this innovation tool.
Additionally, the development of foundation models and large language models is transforming the space. As noted in the 2025 AI Index Report from the Stanford Institute for Human-Centered AI (HAI), the trend is moving from narrow AI models to more comprehensive systems that can handle diverse tasks, from diagnosis to managing clinical notes. This makes the landscape for a specialized the system algorithm that much harder to navigate.
A Critical Analysis of the DCNN-WOA Model
Now, let’s turn a skeptical eye the DCNN-WOA paper. The 97.8% accuracy figure is, on its face, extraordinary. However, the devil is in the details. The model was tested on a publicly available MRI dataset from Kaggle. While useful for academic benchmarking, these “clean” datasets rarely reflect the messy reality of clinical practice, which involves images from different machines, patient demographics, and scanning protocols.
A significant concern is the model’s generalizability. A systematic review of deep learning in medical imaging found that high accuracy in lab settings often overestimates real-world performance due to methodological variations and a lack of diverse data. The reliance on a single public dataset means the DCNN-WOA model’s performance on “in-the-wild” data from a different hospital is a major question mark. This is a frequent failure point for many promising it projects.
A second area for investigation, while the paper claims to outperform other architectures, the real-world value of a the platform tool isn’t just about raw accuracy. Experts have noted that workflow integration, cost-effectiveness, and trust are paramount. An AI tool that is difficult to use or doesn’t integrate seamlessly into existing hospital systems provides little value, regardless of its accuracy. The DCNN-WOA paper, like many academic works, does not address these vital implementation challenges.
Read also: Ai cybersecurity: A Critical Threat to Modern Manufacturing
The Regulatory Bottleneck for ai in medical Tech
Even if a the technology model proves to be robust, a monumental hurdle remains: regulatory approval. In the United States, any software intended for diagnosis is considered a medical device and is regulated by the Food and Drug Administration (FDA). As of early 2026, the FDA has authorized 1,451 AI-enabled medical devices, with radiology tools making up the vast majority (about 76%). This number, while growing, highlights the strict process involved.
The regulatory pathway emphasizes patient safety, clinical validity, and transparency. Manufacturers must provide extensive documentation on their algorithm, training data, performance across different populations, and plans for post-market monitoring. The “black box” nature of some deep learning models presents a serious challenge here. Regulators and clinicians need to understand why a model made a particular this innovation diagnosis, a feature known as explainability, which is not a focus of the DCNN-WOA paper.
Recent guidance indicates, not easier. The agency is moving toward a “Total Product Lifecycle” approach, requiring continuous monitoring of AI models after they are deployed. This is especially true for adaptive algorithms that learn over time. This careful balancing act means that even the most technically brilliant the system algorithm could take years to reach patients, if it ever does.
The Bottom Line on ai in medical
In summary, the DCNN-WOA hybrid model for it detection is an interesting piece of academic research, but it is far from a proven clinical breakthrough. The 97.8% accuracy claim, while eye-catching, is based on a clean public dataset and does not guarantee real-world performance. The actual challenges in this field lie not just in algorithmic innovation but in clinical validation, seamless workflow integration, and navigating the demanding regulatory landscape. The idea that AI will simply replace radiologists is a persistent myth; the future is about collaboration, where AI acts as a powerful assistive tool.
Critical Signals to Watch:
- Key signal: Studies that validate the platform models on large, multi-institutional, and diverse patient datasets, as this is the true test of generalizability.
- A critical development: The adoption of “explainable AI” (XAI) techniques that allow clinicians to understand the reasoning behind an AI’s diagnostic suggestion.
- A key trend: The number of AI medical devices receiving FDA clearance via the rigorous Premarket Approval (PMA) pathway, not just the less stringent 510(k) clearance.
- A crucial metric: Real-world economic studies demonstrating that a given the technology tool is not just accurate but also cost-effective in a clinical setting.
- Note: How major players like NVIDIA and academic hubs like Stanford HAI incorporate or respond to these niche optimization techniques within their broader, more established frameworks.
At this moment, the hype around this specific ai in medical model outpaces the evidence. Skeptical observation remains the correct posture.